Lesson 5: Change
Attention
plus ça change, plus c'est la même chose
Bon Jovi - The More Things Change
Click HERE to view this directly on YouTube
Learning Outcomes
Upon completion of this lesson's material, students will
- Understand the Stages model as applied to Disease, Change and Recovery
- Be able to define "transtheoretical" and state advantages and disadvantages of this method of conceptualization
- Be able to state at least one other way of thinking about how change takes place
- Understand the role of Motivational Interviewing in enabling progress from precontemplation to contemplation
- Be able to state what change processes are helpful at various stages
Readings
Chapters 8 and 9 in The Thirteenth Step
YouTube video: https://www.youtube.com/watch?v=_KNIPGV7Xyg
Teaching
Change. How and when and why it happens and how we can help the process. Stages of disease, stages of recovery and stages of change.
Change---the transtheoretical perspective
Developed by Prochaska and DiClemente at the University of Rhode Island in the mid-1970's
Transtheoretical implies that this way of looking at change fits any theoretical orientation, e.g. learning theory, psychodynamic theory, etc. It asserts that change takes place as described regardless of who is the helper, who is being helped or what is the behavior under consideration. Originally developed around tobacco smoking cessation.
Has a positive hopeful view of human nature---that people will make the right decision if given good information and time and space to think about it. Works well with non-directive counseling and motivational interviewing (Be sure to read this carefully and to watch the YouTube video in the readings section which models a motivational interviewing technique called OARS: you have a Book Quiz this week on Motivational Interviewing)
Different from AA which says we have to touch bottom and acknowledge powerlessness before we are ready for change. Teaches us simply to consider what's best for us at any given time and place and to use what power we do have to make our life better.
Also different from insight oriented theories which see a sudden breakthrough to a new level of understanding (e.g. Gestalt and other insight oriented therapies such as Freudian and Jungian psychoanalysis). Here the change takes place often after much effort in a sudden flash of enlightenment.
Religious conversion may also emphasize sudden change typically occurring as a supernatural event (e.g. "born again"). There may or may not be a period of striving (repentance, conviction), but the change is not gradual or stage based and often is seen as not depending on human effort.Stages of Change
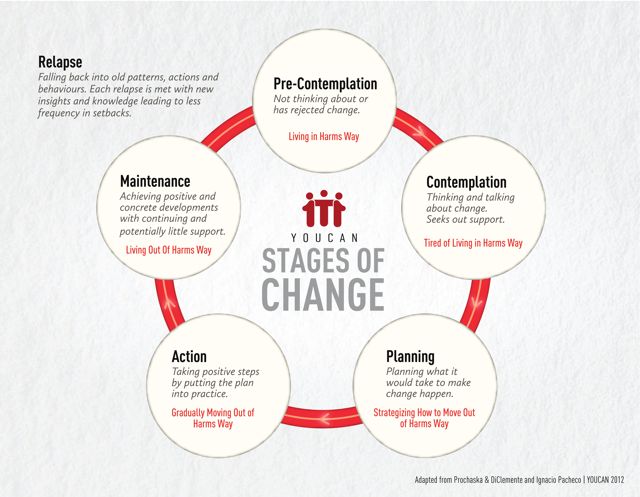
Precontemplation - don't see a problem. No change planned on the next six months.
- The five "Rs" Reveling, reluctance, rebellion, resignation and rationalization
- May enter treatment to placate others
- Denial and resistance addressed through Motivational Interviewing (MI) which uses open questions, affirming, reflecting and summarizing. Rolls with the resistance
- Goal is to help person move from precontemplation to contemplation
- Change processes are consciousness raising, emotional arousal/dramatic relief, self-reevaluation, environmental reevaluation
- It's ok to end counseling after a session or two if there is no movement which preserves the person's autonomy and shows respect for them thus keeping the door open for future contact
Contemplation---thinking about it. Change contemplated in the next six months.
- Ambivalent
- Evaluating pros and cons, risks and benefits
- Change processes are self-revaluation, environmental reevaluation and social liberation
- May return to precontemplation or be ready to move on to preparation
Preparation/Planning---making a plan and finding resources
- Ready, willing and able
- Change processes are self-liberation, stimulus control, counterconditioning and helping relationships
- Increase self-efficacy. Ways to do that: remind client of past success with change, show him/her examples of other people with whom s/he identifies succeeding at change, help client to construct a plan for change that begins with baby steps which s/he has already mastered
Action---doing something about it. Making the change.
- Committed
- Change processes are self-liberation, stimulus control, counterconditioning, reinforcement management and helping relationships
- May be involved in cognitive behavioral therapy, 12 step program, Rational Recovery, or other therapies or programs to help make the change
Maintenance---keeping the change
- •Avoiding lapses ( slip or two) and relapse (a pattern of slips). Learns to deal with cravings by doing something else, waiting it out (which works because the craving occurs in the presence of something that reminds the person of the old habit and time will reduce the craving through the process of exposure/extinction), or meditating to reduce the salience of the desire for the old habit.
- Building new lifestyle (change in friends, change in activities that remind one of the old habit, beginning to focus on new habits that lead to more of a sense of self-fulfillment) that maintains the change
- Change processes are the same as for Action with the addition of social liberation •
- BOTTOM LINE: NEW HABITS FOR OLD.
Stages of Disease
Model used in medicine for diseases that are chronic, progressive and sometimes terminal
When applied to SUDS, implies a biological basis that may have psychological and social and cultural and spiritual dimensions but that is basically biological in cause and management and cure when possible
Example is diabetes which is a problem with insulin production in the pancreas. We can't cure it but we can manage it through medication, weight loss, exercise and diet change
Some experts make a distinction between use of substances that causes problems and true dependence (with preoccupation, loss of control and compulsion to use) . Only persons who are "dependent" have a disease in this view while problem drinkers just need counseling to change bad habits.
Other experts (e.g. Jellinek) see use with problems in a continuum with the dependent phase. Jellinek developed a curve illustrating the stages of the disease of alcoholism and the stages of recovery (Just as a note, Jellinek’s thinking changed throughout his life so that at different points, he advocated different views than those depicted here).
Stages of disease dovetails with Stages of change model in describing how recovery takes place. But, as a reminder, Stages of Change differs from AA (which often appeals to the Jellinek curve) in that the Stages of Change model does not require the person to "touch bottom" or admit powerlessness or surrender to a higher power.
Addiction and Recovery - The Jellinek Curve
Diagnostic and Statistical Manual
- DSM V seems to eliminate the distinction between "Abuse" and "Dependence" and subscribe to Jellinek's view of substance use issues as a single continuous curve from mild to moderate to severe
- DSM V says "Abuse" was eliminated because of lack of inter-clinician agreement in trying to make the diagnosis
- The criterion of “Legal Problems” which was part of the Abuse diagnosis was dropped from DSM 5 perhaps to continue the decriminalization of substance use disorders differentiating them from problems in living associated with substances but which are not neurophysiological in origin and do not require psychiatric treatment (e.g. drunk driving, peddling drugs)
- In making these changes, DSM 5 seems to be moving towards a model of addiction that is more biological and less interested in legal or criminal aspects of use
Stages of Recovery
- Recognizes that there are different tasks in Early, Middle and Late Stage Recovery
- Early Recovery
- Traditionally in Early Recovery in AA the counsel is to do "90 in 90", be selfish and just focus on staying clean and sober, and to just do the 1st three steps of AA involving surrender and "turning it over to the Higher Power"
- Stages of Change model would see Early Recovery (and to some extent Middle) as the Action Stage, changing habits that don’t help for ones that do
- Middle Recovery
- Middle Recovery in AA involves steps Four through Ten, taking inventory and repairing damaged relationships and trying to start fixing what was broken while drinking or drugging was going on.
- AA would see Middle Recovery as beginning about the Fourth Month and continuing for six to nine months
- Change processes in Middle Recovery in the Stages of Change Model are like those in the Action and Maintenance stages and involve gradually learning to end lapses and keep that change for the better
- Stages of Change sees Maintenance as starting by the sixth month.
- AA doesn’t have a maintenance stage but sees a similar concept in Late Recovery
- Late Recovery
- Late Recovery is the flourishing of the clean and sober person as he or she begins to reap the benefits of recovery establishing a new lifestyle built on sobriety rather than substance use
- In AA would usually not be seen as beginning until the second year of sobriety
- In Transtheoretical Model this would be the Termination Stage where temptation is minimal and the new behavior is solidly entrenched.
- AA does not have a Termination Stage: since the disease is chronic the person is always “recovering” never “recovered”.
- Relapse Prevention
- Traditionally relapse prevention is the primary task for the first six months or so,
- Relapse prevention includes teaching the client how to deal with cravings and also how to discern warning signs of relapse and prepare plans to prevent relapse.
- Typical warning signs follow the acronym HALTS
- Hungry/thirsty
- Angry
- Lonely
- Tired
- Stress
- The prevention plan for each is to deal with the warning sign appropriately, e.g. by eating, calming, socializing, resting, meditating
- Stress is particularly important in causing relapse during the first year of alcohol recovery perhaps because the drinker’s nervous system is still getting back to normal
- Each client must also prepare his or her personal warning sign list based on previous attempts (if any) to change the problem. An example would be someone who has always lapsed around pay day. The plan would be what to do (e.g. go to a movie with a sober friend) instead.
- Making a relapse prevention plan based on managing warning signs has been particularly advocated by Terrence Gorski

Assessment

Lesson 5 Quiz
- List the change processes in the Contemplation Stage as mentioned in the Lesson. Give an example of each (you can find examples by clicking on “change processes” link in the Lesson). (20 points)
- List 3 alternatives that were mentioned in the Lesson to the transtheoretical model. Give an example of each.(20 points)
- Describe as mentioned in this Lesson how DSM 5 sees SUDs and how that is different from DSM 4.(20 points)
- Give examples of what is expected by AA in Early, Middle and Late Stage Recovery and compare and contrast AA’s view to the Transtheoretical view. (20 points)
- Follow the link in the Lesson for Motivational Interviewing. List the Five Principles of Motivational Interviewing. (20 points)
Lesson 5 Assignment
Create an audio-visual presentation in YouTube comparing and contrasting the 12 Step approach to another approach of your choice. Talk about how change takes place in each approach, especially considering the initial decision process and ensuing implementation of the process of change. Conclude the presentation by saying which approach you prefer and why.
For this assignment you are going to create a visual presentation with a voice over recording. You will be using an app called Adobe Spark Video
|

Lesson 5 Discussion
Describe a bad habit you have tried to change. Describe how the transtheoretical model worked in your case and what stage of recovery you are currently in and why.