Lesson 4: Psychological, Social, Family, Culture, and Spiritual Issues
Attention
Bag of Tricks These Internet sites will help you in this class especially in writing essays and assignments. They are good sources of information and will help you also in your work and continued learning after graduation. Substance Abuse and Mental Health Services Administration Store EROWID - Documenting the Complex Relationship between Humans and Psychoactives ProCon.org - Explore Pros and Cons of Controversial Issues Medical News Today |
Learning Outcomes
Upon completion of this lesson's material, students will
- Understand and be able to discuss psychological, social, cultural, family and spiritual factors that contribute to SUDs
- Begin to understand and be able to state the current limits on our knowledge about SUDs
- Be able to discuss in a rational, logical and respectful way differences of opinion about SUDs
Teaching
PSYCHOLOGICAL CONSIDERATIONS
Is there a personality that predisposes to SUDS?
Some within the AA community deny that there is a specific personality type that predisposes individuals to SUD. The Betty Ford Center, for example, claims there is no connection.
One advantage of this perspective is destigmatization: “Anyone can be an alcoholic or drug addict.” But DSM 5 asserts that impulsivity and a history of conduct problems are risk factors for many SUDs. The question is whether these temperament traits are genetically and physiologically connected to addiction or whether the relationship is more tenuous with several different temperaments possibly associated with addiction. The jury is out. Here’s another website that summarizes the complexity of the debate.
Bipolar Disorder, Schizophrenia, Anxiety Disorders and Depressive Disorders have higher rates of SUDs than for the general population. The question is: what is the direction of the relationship? Are people with these disorders medicating their symptoms or has use of substances caused the disorder? There is, for example, evidence that heavy adolescent use of cannabis is associated with higher rates of psychotic disorders and that it is probably the substance’s action on the brain causing the disorder.
Learning models of addiction emphasize the roles of classical and operant conditioning from first use to full blown addiction. These models also emphasize cognitive behavioral interventions to reduce or eliminate substance use. Classical conditioning (like with Pavlov’s dogs) is involved in craving and in the initial learning that use of a substance will give pleasure. For example, smoking a substance gets it to the brain quicker and deepens the association between the substance and the sense of pleasure so that it is harder to quit. Operant conditioning (habit formation) is involved in the lifestyle choices we make that support substance use (who we use it with, when we use it, how we use it). To change substance use, ultimately we have to learn a whole new set of habits: what do we do to wake up, to relax, to celebrate, to socialize, to concentrate, etc., etc. This model emphasizes cognitive behavioral interventions to reduce or eliminate substance use.
Social Considerations
Social Learning Theory posits that we learn our behaviors from our environment as they are reinforced by important people in that environment...thus many problems become associated with certain kinds of environments.
Socioeconomic concerns, especially the question: Does poverty cause SUDS or do SUDS cause poverty? The answer is “both”.
Social factors that may contribute to SUDS: Family influence, peer influence, influence of other social systems. (school, church, internet social applications, etc.).
The DARE (Drug Abuse Resistance Education) program which has been widely used in elementary schools emphasizes refusal skills based on fear of legal consequences and education about the effect of drugs and alcohol. DARE is associated with “just say no” thinking and there is much evidence that it is not particularly effective in reducing youth substance use. Since 2009, DARE has been using a modified approach called “Keepin’ it REAL” which may be more effective although the DARE version has not been empirically tested.
There is considerable evidence that two factors that strongly influence adolescent substance use are parental modeling and clear and consistent parental rules.
The conclusion is that helping families escape poverty and parents to make good choices and to teach their children to make good choices reduces substance use problems.
FAMILY CONSIDERATIONS
Is there a typical alcoholic family structure?
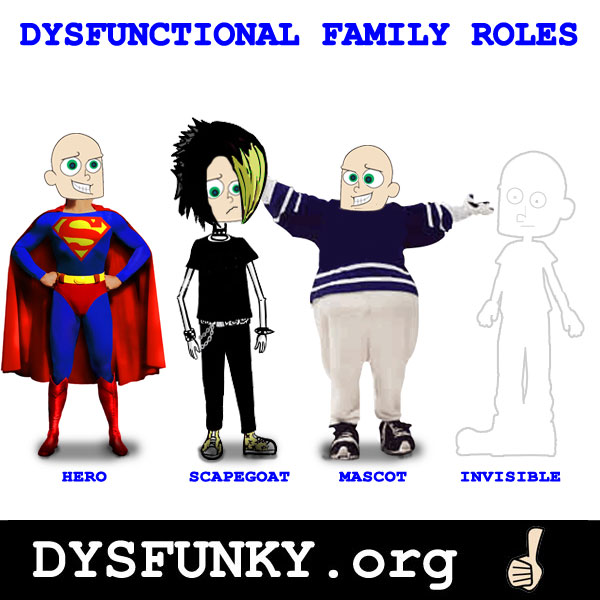
The Family Therapy movement of the 1970’s contributed to the concept of typical roles in a family with an alcoholic parent. Click HERE for an article on the "Roles in the Addicted Family System"
Adult Children of Alcoholics (ACOA) a 12 step recovery group for family members talks about alcoholic family rules: “No Talk. No Trust. No Feel”. Another 12 step recovery group Al-Anon emphasizes the "Three C's"...
“We didn’t cause the drinking and we can’t control or cure it”
...and counsels family members either to leave or if they stay to detach from the alcoholic and “keep the focus” on their own well-being.
A different emphasis is made by practitioners of Community Reinforcement and Family Therapy (CRAFT) who practice differential reinforcement of behaviors that replace substance use while quietly and consistently encouraging the user to join in therapy. For example a wife might reward her heavy drinking husband for coming home earlier rather than spending time with drinking buddies. She would also point out that things seem to go better at home when he drinks less. Finally she would help him connect to treatment if and when he is ready.
The bottom line is that the family has great power to contribute to substance use and also to help people leave substances behind.
Co-dependence is a concept that emphasizes an unhealthy relationship may develop with a substance user. The user is dependent on the substance and the codependent is dependent on finding their self-esteem and self -worth in caring for the user.
As helpers, MHRT/Cs are at risk of becoming codependent!
Risk is reduced by developing healthy self-esteem that comes from within rather than the approval of others: the goal is “interdependence”---that we can be in caring relationships while maintaining our own identity and self-worth.
CULTURAL CONSIDERATIONS
SUDS incidence rates among different ethnic groups.
See especially tables 1 and 2 that summarize differences between different groups of humans. Some differences in substance use are biologically based. For example, many Japanese lack the gastric enzyme alcohol dehydrogenase and consequently have a profound uncomfortable flushing response when they drink and as a result may be less susceptible to alcohol use disorder. Women also may be more likely to have lower levels of this gastric enzyme.
International differences in SUDS (2004)
As you can see, alcohol use is much higher in Eastern Europe and South America and in the U.S. and Western Europe than it is in Arab countries and much of Africa
Jewish (Israel) and Islamic (North Africa, Middle Eastern Countries, Indonesia, Pakistan) people generally have lower SUDs rates than Christian countries (U.S. Ireland, France, Italy, Russia) although for example there is a big difference between Irish AUD rates and Italian AUD rates (both “Christian” countries) perhaps because Italians generally frown on drunkenness. These differences reflect different attitudes towards drinking and intoxication in the various religious groups.
SPIRITUAL CONSIDERATIONS
Generally “spiritual” refers to the area of human life that deals with values and purposes
Religion on the other hand is the social and cultural embodiment of those values and purposes
We have already seen that the religions of Judaism and Islam seem to foster attitudes towards substances that reduce SUDs. Islam generally forbids substance use (like Mormons). Judaism emphasizes the sacramental use of wine as a part of daily life and as in some Christian countries (Italy) drunkenness is seen as disgraceful. When these attitudes are deeply embedded, they can have a protective role even when the religious adherent participates in a culture that uses substances recreationally
Alcoholics Anonymous' 12- Step Program says it works by “turning it over to a Higher Power”
The model of the 12-Steps has been adopted by many groups related to addiction including substances, sex, and gambling.
A different, but related, approach is seen in Logotherapy, a therapy developed by Victor Frankel, a Jewish survivor of the Nazi extermination camps who observed that people who survived the holocaust did so because they had values that transcended mere survival and gave purpose even in the terrible surroundings of the concentration camp.
Assessment
Lesson 4 Assignment
You will be creating a family history document. This lesson shares that a good understanding of one's family history is a very important part of the Comprehensive Assessment that we do with all SUD clients. This is because 40% to 75% of the risk of developing a SUD is genetic. At this point a family history covering at least three generations is an even better predictor of SUD risk than genomic sequencing.
Compose your family history including grandparents, parents and children (if any). Indicate whether there are or were substance use issues for each person.
Here is an example for you to follow:
Your client’s name is John Doe. He is 45 years old and has diagnoses of Bipolar Disorder and Alcohol Use Disorder in sustained remission (last drink was two years ago). He is married to Jane Doe (40yo) and has been married to her since 1990. They have three children: Jim Doe (23) who drinks a lot and has had two OUIs already, Jean Doe (21) and Joe Doe (19). John’s parents are Jeb (70) and Jacquie (65). Jeb is a recovering alcoholic with 30 years of sobriety and Jacquie has no history of substance use. Jeb has had recurrent depression but it has improved with abstinence. Jeb and Jacquie have another son, Justin (40 yo) who has been treated for heavy drinking and who is currently in relapse. Jane Doe has no history of substance use and her parents are Don and Darlene Smith. Don is 65 and is a social drinker and Darlene is 64 and has a glass of red wine daily as suggested by her physician. Jane was an only child.
Here is the genogram that reflects this history.
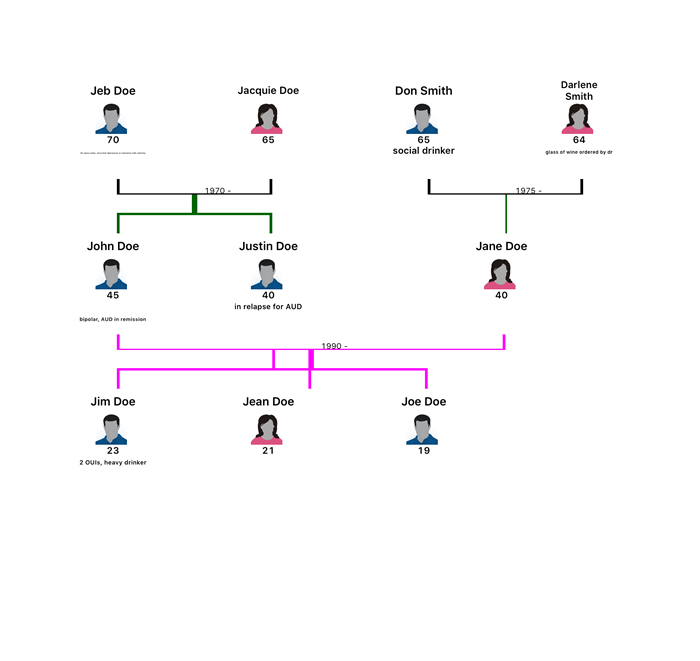
As you can see, for Jeb Doe the information is unreadable without magnification because of the software I used in creating my genogram. You can probably do better if you find better software. One place to look is in Word where you can find several templates for creating genograms by typing "family tree" into the search engine. You will need to submit your homework as a PDF file so whatever software you use, make sure it can save your final product as a PDF. Please email your instructor if you have additional questions abou this project.
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
Lesson 4 Discussion (For online students only)
Write a paragraph stating what your experience leads you to think is the best approach to dealing with addiction. Why? Write another paragraph saying what you think is the worst approach. Why?