Lesson 6: Nicotine Use Disorder
Attention
Produced by Cherokee Nation Healthy Nation, this video explains the sacredness of traditional tobacco and the fact that use of commercial tobacco is not sacred in Native American or Cherokee culture. Take note of the claim, not supported by evidence, that native tobacco is healthier.
Click HERE to view this video directly on YouTube.
Learning Outcomes
Upon completion of this lesson's material, students will
- Understand how Tobacco Use Disorder helped to inspire the work of Prochaska and DiClemente
- Understand the concept of "self-medication" and how it affects tobacco users
- Be able to state how Tobacco Use Disorder reflects the limits of the Stages of Change model
- Understand how nicotine works to produce addiction
- Be able to state reasons why some addictive substances are legal and others are not
- Be able to discuss smoking cessation with MHRT/C clients and to assist them in cessation
Teaching
NICOTINE USE
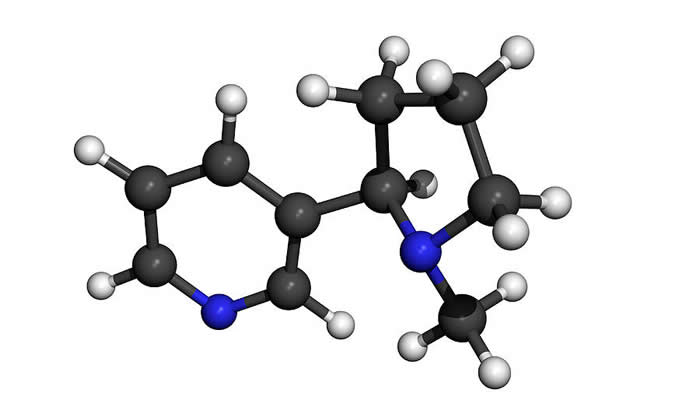
Molecular Model of Nicotine
- DSM 5 calls it Tobacco Use Disorder perhaps because nicotine replacement plays such an important role in treatment. But we will refer to it as Nicotine Use Disorder (NUD) because nicotine is the addictive substance and now with e-cigarettes, people are using nicotine without tobacco. Also calling it Tobacco Use Disorder would be like referring to alcohol addiction as "Wine Use Disorder" or "Beer Use Disorder".
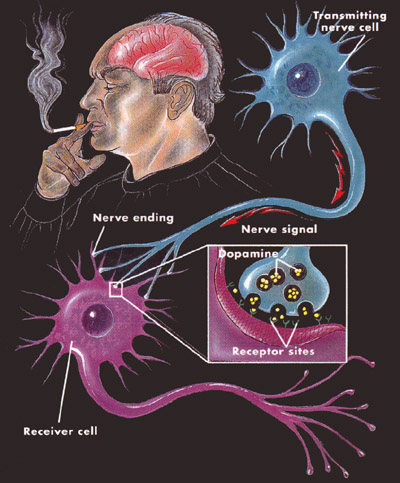
- Nicotine is a cholinergic receptor agonist. It works through stimulating production of the neurotransmitter acetylcholine which is the most widely distributed transmitter in the body. Acetylcholine is especially important in muscle function. As such nicotine can both increase muscle activity and activate the parasympathetic ANS producing relaxation. Nicotine is therefore the "renaissance drug" producing both stimulation and relaxation. Stimulation usually occurs at lower doses and relaxation at higher doses. Nicotine is very toxic. The average dose in a cigarette is 2mg. The LD50 dose in humans is just 40 to 60mg. Nicotine like many other substances produces other neurotransmitters as it works its way through the body. Most significant is epinephrine (adrenaline) which is also released by cocaine, amphetamine and caffeine. Epinephrine is the second most widely distributed mediator in the body and works especially by stimulating the sympathetic nervous system giving people a sense of excitement and alertness. Finally nicotine use results in the release of dopamine in the basal ganglia and especially the nucleus accumbens which produces a sense of pleasure and reward.
- Most other substances (including alcohol, opiates, cocaine, marijuana, benzodiazepines, barbiturates) also finally cause the release of dopamine in the nucleus accumbens and this is the final common pathway of addiction. Without this mechanism of stimulation of the basal ganglia through dopamine activity, addiction would not occur.
- Thus tobacco use is a model for all other addictions.
- Smoking can be seen as a very tough addiction to work with because:
- Smoking any substance is the fastest way to get the substance to the brain (even faster than intravenous injection) and the faster it gets to the brain and produces pleasure the more likely that classical conditioning will occur and produce learning that is hard to reverse
- As mentioned, tobacco both relaxes and stimulates so it becomes a ubiquitous habit
- The harm caused by tobacco takes many years to accumulate so that even though it finally causes more sickness and death than all other substances combined, it is hard to sustain motivation to quit when strong cravings occur
- Statistics show that half of smokers though they try their hardest will never be able to “kick the habit” and that most smokers have to try many many times to make it work.
- So if you can help a smoker to quit, you can work with any addiction
Legal vs illegal Substances
- Currently legal: alcohol, tobacco, caffeine. Also dextromethorphan, diphenhydramine, nutmeg, morning glory seeds, glue, gasoline, nitrous oxide, poppers etc. etc.
- EROWID is a resource for understanding why people use substances. Look up nutmeg on Erowid and see why people use it to get high.
- DEA Schedule: Part of the Controlled Substances Act signed into law in 1970. The legislature ignored the suggestion of the Shafer commission to decriminalize marijuana and instead put it in Schedule 1 which prohibited any use, denying any medical or other efficacy. The Schedule Level is supposedly determined by medical utility and abuse potential, but cannabis’ placement in Schedule I is puzzling because it had a history of medical efficacy (even the American Medical Association had suggested keeping it in the pharmacopeia) and experts of the time did not consider it particularly harmful in itself though they thought it might be a “gateway drug” to worse substances. This issue illustrates how drug scheduling and whether they are legal or not is as much a matter of politics as it is of medicine. Legal drugs like tobacco and alcohol are not scheduled or even subject to Food and Drug Administration oversight but rather are dealt with by the Alcohol Tobacco and Firearms agency. Recently there has been some effort to put nicotine under the oversight of the FDA.
- One outcome of placing cannabis in Schedule I is that it has made it difficult to do research on it. To get samples for research, scientists had to get them from the National Institute on Drug Abuse which rarely granted access. Tobacco and alcohol on the other hand have been widely researched because they can be freely obtained and because there has been little stigma associated with their use.
- The research that has been done clearly demonstrates that tobacco is the most harmful substance used by humans causing more sickness and death than all other substances combined. A pack a day smoker has about a 40% chance of dying of a smoking related disease. But the public doesn’t get as distressed about tobacco as they do about heroin or cocaine because it takes much longer to see the harm caused by tobacco.
- Harrison Narcotics Act. (1915) Designed to regulate use of narcotics which had previously been freely available in the U.S. As with alcohol prohibition which came soon after, the Act was sold to improve the health and morals of the nation but the politics of the time traded on fears of use by drug crazed minorities.
- Marijuana Tax Act.(1937) Although it only taxed marijuana its effect was to result in self-incrimination under state and Federal Laws if the tax was payed. Supreme Court finally found it unconstitutional in 1969 but was immediately replaced by the Controlled Substances Act. The laws arguably were sold to legislators and to the public based on perception of harm greater than that of the legal substances alcohol and tobacco and the perception that use was largely confined to antisocial elements of despised minorities.
- Compared to other drugs, nicotine is by far the greatest threat to health. CDC - Fact Sheet - Tobacco-Related Mortality - Smoking & Tobacco Use
Tobacco use in Special Populations
Smoking rates vary from about 20% of the general U.S. population (down from about 50% in the 1950's). Smoking rates much higher for people with a substance use or mental illness diagnosis with 44% of U.S. consumption by this population. Rates vary by diagnosis with highest rates for Schizophrenia and Bipolar (50 to 70%) and for Alcohol Use Disorder (upwards of 85%). People with anxiety and depression smoke at about a 40% rate.
- People with Schizophrenia may be self-medicating the negative symptoms of schizophrenia (especially anhedonia, poor social interaction). Tobacco use may also improve cognitive function although nicotine use can aggravate the thought disorder in schizophrenia producing an increase in hallucinations
- People with anxiety and depression look to the relaxing and stimulating effects of tobacco.
- Tobacco smoking may interact with alcohol to potentiate the effects of both.
QUTTING SMOKING

Click the logo to visit the website for Tobacco-Free Maine
Trying to quit
- The Stages of Change Model was developed around helping people to stop smoking. The primary issue with any addiction but especially smoking which in many ways is the hardest to change is to raise consciousness of the pros and cons of continuing the habit. The appeal always is to "What's best for you?" trusting the person to sort that out for themselves This is the opposite of the confrontation techniques that were so widely used with addictions even a few years ago.
- Motivational Interviewing is used to help the person move from Precontemplation to Contemplation and from Contemplation to Preparation. The Interviewer rolls with the resistance rather than confronting it. MHRT/Cs can be especially helpful as trusted advocates for the client who consciously dedicate their work to helping the client actualize their full human potential. The MHRT/C as community support worker helps the client to plan improvements to their life while as case manager they help the client to marshal their resources.
- Even with Stages of Change and Motivational Interviewing only 50% of smokers succeed in quitting even with multiple attempts. Best advice is to "Keep on quitting!" but people grow discouraged because this addiction is so hard to overcome.
- The limits of Stages of Change is that it depends on resolution of ambivalence and strong motivation to make the needed efforts at change. Repeated failure despite one’s best efforts can cause a loss of hope. Believing in one’s ability to change can be difficult for folks who have not had a lot of success in life and have had a lot of trouble. Also difficult for depressed people.
Medications that Can Help
Nicotine Replacement Therapies. The patch has been around since the 1960's and is the original medication assisted therapy (like suboxone or methadone for Opiate Use Disorder). Like methadone and suboxone it is designed to reduce harm rather than to cure the addiction. So people using nicotine replacement are still addicted to nicotine but less likely to die of cancer or heart disease because it is tobacco which is harmful, not nicotine. Nicotine does raise heart rate and blood pressure but the effects are transitory and there is only a slight increase in heart problems with nicotine used without tobacco. The patch reduces harm by reducing exposure to tobacco carcinogens and also by changing dosing schedule from one controlled by desire to use to one controlled by steady release of nicotine: when this happens it is easier to eventually reduce and finally stop use altogether. So the patch starts with a dose equivalent to about a half pack a day and tapers down over several weeks.
Nicotine now also available in gum, lozenges, puffers, nose spray and e-cigarettes (all of which are FDA approved except for the e-cigarettes). These forms of nicotine replacement have the disadvantage of being used when the person who is trying to quit has a craving and thus continue the link between craving and use.
Zyban. This is Wellbutrin (bupropion) marketed for smoking cessation. Mechanism of action is unknown but may be related to release of epinephrine and dopamine in the limbic system.
Bupropion (Zyban) for Quitting Smoking
Chantix. A nicotine receptor blocker that makes the person feel like they have just had a cigarette. Reduces craving to the point where the person does not want to smoke. Is taken for 12 weeks and may produce quit rates as high as 40%
Alternatives to Smoking (e-cigarettes and vaping)
The use of e-Cigarettes and Vapor options are on the rise. Many people have had great success substitution these seemingly less harmful habits for their smoking.
Here is an article and Vaping from Vaping360 (certainly a website in FAVOR of vaping)
Vaping is not without its concerns though...such as the one expressed in this article Concerns explode over new health risks of vaping. (Although, I'm not sure how "explosive" this set of concerns has been!
Treatment that Can Help
- Cognitive Behavioral Therapy. Helps the person learn new coping skills to maintain abstinence. Helps them to replace the habits of addiction (where they smoke, when they smoke, under what circumstances they smoke) with new habits that meet their need without the chemical. For example waking up to a brisk walk rather than a cigarette to get your body going. Relaxing with deep breaths rather than smoking.
- Support Groups . Not as successful with this population as with AA and NA. But social approval from friends and family can be powerful.
- Traditional attitude of AA towards smoking cessation has sometimes been negative - discouraging alcoholics from trying to change too much at once. But increasingly research demonstrates that people who quit smoking at the same time they quit drinking are more successful in changing both habits, perhaps because the heavy association of smoking with drinking triggers cravings, perhaps because of general down regulation of dopamine in the nucleus accumbens by stopping both chemicals.
Assessment
In this section you will find a list of the required Assessments that accompany this Lesson. The Lesson Discussions are designed for the ONLINE and HYBRID versions of this course. If you are not in an ONLINE or HYBRID version of this course you can ignore these instructions unless otherwise guided by your instructor.
Lesson 6 Quiz
- Describe one mental illness where a smoker may be self-medicating. What are the symptoms that are being medicated? (20 points)
- List the reasons given in this Lesson why the Stages of Change Model may encounter difficulty helping people to change their smoking habit. (20 points)
- List the neurotransmitters involved in tobacco use. What are the behavioral effects of each one? (20 points)
- List two factors influencing whether a substance is legal or illegal. (20 points)
- What DEA schedule is cannabis in? How does this influence research? What DEA schedule is alcohol in? How does this influence research? (20 points)
Lesson 6 Discussion
Describe how you as an MHRT/C could help a client who smokes and has emphysema. What is your likelihood of success in helping them achieve permanent abstinence and given this factor how might you change your approach?
Research iPad apps that are related to smoking. Select a specific app, name and describe it, and explain how you might use that app with a client.